How to Use TiC Data to Demand a Rate Increase

Most practices can feel it in the numbers. Collections lag. Certain CPTs are weirdly low. One payer pays fine for office visits but absolutely punishes procedures. And then you hear the practice across town is getting 30 percent more for the same work. The problem is not just that the rates are low. It is that the negotiation is lopsided.
Payers show up with spreadsheets, “market rationale,” and a calm tone that basically says, this is the going rate. Practices show up with a few remits and a lot of frustration.
However, [Transparency in Coverage data](usually called TiC), is one of the first real chances independent practices have had to flip that dynamic. Not by yelling. Not by begging. But by walking in with market anchored evidence.
This is a practical guide to doing exactly that.
What TiC data actually is (and why payers quietly hate it)
TiC files are public machine readable files that many health plans and issuers are required to post. Inside those files is negotiated rate information tied to billing codes. In other words, not just “allowed amounts” from your own claims. Actual contracted rates that exist in the market.
There are a few caveats, and we will talk about them. The files are messy, enormous, inconsistent, and easy to misread. But the important part is this:
TiC lets you stop arguing from your experience and start arguing from the market.
If your payer says, “We cannot do better than 108% of Medicare on 99213,” you can respond with, “In this same county and product type, rates cluster around 140 to 165% of Medicare for comparable providers. Here is the range. Here is where you have us.”
Different conversation.
The negotiation mindset shift: you are not asking, you are correcting a variance
This matters more than people realize.
If you approach negotiation like, “Please increase our rates,” payers can dismiss it as preference.
If you approach it like, “Your rates for our contract are materially below local market benchmarks for the same services,” it becomes a variance correction. A mismatch. Something that requires explanation.
TiC data is basically the receipt.
Step 1: Pick the right codes to benchmark (do not benchmark everything)
A common mistake is trying to renegotiate the whole fee schedule at once. It sounds bold. It also makes it easy for a payer to stall, redirect, or cherry pick.
Start with a focused list. Ideally:
- High volume codes (where a small delta becomes real money)
- High revenue codes (where a 10% swing is massive)
- Strategic codes tied to your core services (the ones you do better than anyone)
For many primary care practices, this might look like:
- 99213, 99214, 99215
- 99395 to 99397 (preventive)
- 87086 (urine culture) or common in office labs, depending on setup
For specialties it gets more interesting. Ortho, GI, cardio, imaging, behavioral health. You get the idea.
We usually recommend 15 to 40 CPTs for a first pass. You can always expand later once you win credibility.
Step 2: Decide what “market” actually means for your case
This is where payers love to play games. They will say you are not comparable. Or that the rates you found are not the same product. Or that those are “unique contracts.”
So define market carefully. Think of it like a courtroom. You want comparables.
Your comparables should match on:
- Geography: county, city, or a tight region around your service area
- Provider type: specialty, facility vs professional, site of service
- Billing context: same CPT, same modifier patterns if relevant
- Plan and product: commercial PPO vs HMO, exchange, employer plans. Sometimes you cannot match perfectly, but you can get close enough.
The tighter the match, the harder it is for a payer to dismiss.
Step 3: Pull TiC data (and be honest, it is brutal to do manually)
Let’s just say it plainly. TiC files are not built for humans.
They are often:
- multiple gigabytes
- published in different schemas
- missing helpful identifiers
- filled with rate “types” that require interpretation
If you have a team of software and data engineers and a few months to develop custom software, sure, you can wrangle them yourself. Most independent practices do not.
This is why tools exist that turn TiC into something usable. And yeah, this is exactly the problem Reveon Health was built around.
Reveon Health (https://reveonhealth.com) focuses on making TiC based benchmarks accessible to smaller practices who cannot pay enterprise pricing. The core idea is simple. You should be able to walk into a payer negotiation with credible benchmarks without hiring a consulting firm or building an internal analytics team.
Step 4: Normalize your rates so the comparison is apples to apples
Even if you get clean benchmark numbers, you still have to compare correctly. Otherwise you will get burned in the meeting.
Here are the most common normalization approaches:
Option A: Compare fee schedule dollars directly
This is simplest when you can line up the same CPT and the same contract basis. You present:
- Your current allowed amount
- The payer market range (min, median, max)
- Your target
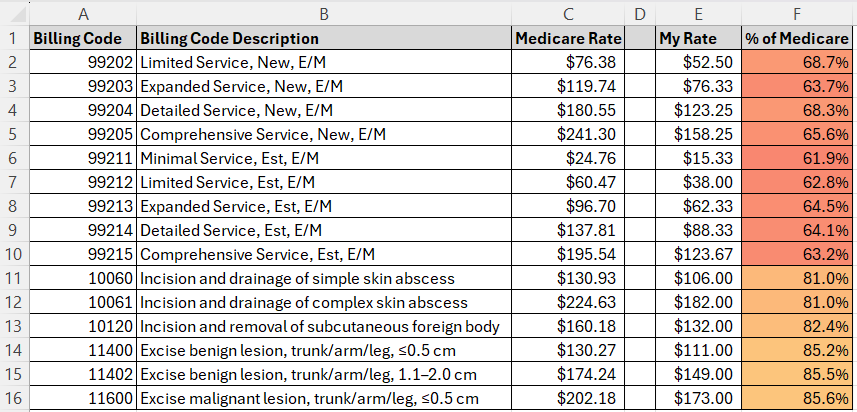
Option B: Convert everything to “percent of Medicare”
This is often the most persuasive because Medicare is a common reference. Even payers use it internally.
You take the TiC negotiated rate for a CPT in your market and convert it:
Commercial Rate / Medicare Rate = % of Medicare
Now you can show:
“This code is paying at 112% of Medicare for us, but local rates cluster at 150 to 175%.”
Option C: Weighted impact
Not every code matters equally. Tie the benchmark delta to actual volume.
Show the payer the annualized impact if they moved you to median, or to the 75th percentile.
That is where the conversation stops being theoretical.
Step 5: Build a benchmark story the payer cannot easily dismiss
Do not just send a spreadsheet dump. It looks like you do not understand it. Build a short narrative.
A strong benchmark story usually includes:
- Your position vs market: “We are below the 25th percentile on 17 of 25 of our core codes.”
- Pattern recognition: “Undervaluation is concentrated in E/M and ultrasound.”
- Reason for correction: access, retention, quality, patient load, shortage area, outcomes. Pick what is true.
- Clear ask: “Move these codes to median market, effective on renewal.” Or “Increase conversion factor to align with X.”
And keep it tight. If you overwhelm them, they will stall.
The charts that actually work in negotiations
You do not need fancy design. You need clarity.
These are the visuals that tend to land:
- Histograph chart per CPT. Shows distribution of market rates, with your rate highlighted as a marker.
- Percent of Medicare scatter plot. Each point is a CPT. You are the red dots, market median is the line.
- Revenue impact table. “If moved to market median, estimated annual increase: $___.”
- Top 10 underpaid codes. Sorted by dollars lost per year, not just percent difference.
Some example images are shown below.
Image: Sample “Your Rate vs Market Range” chart
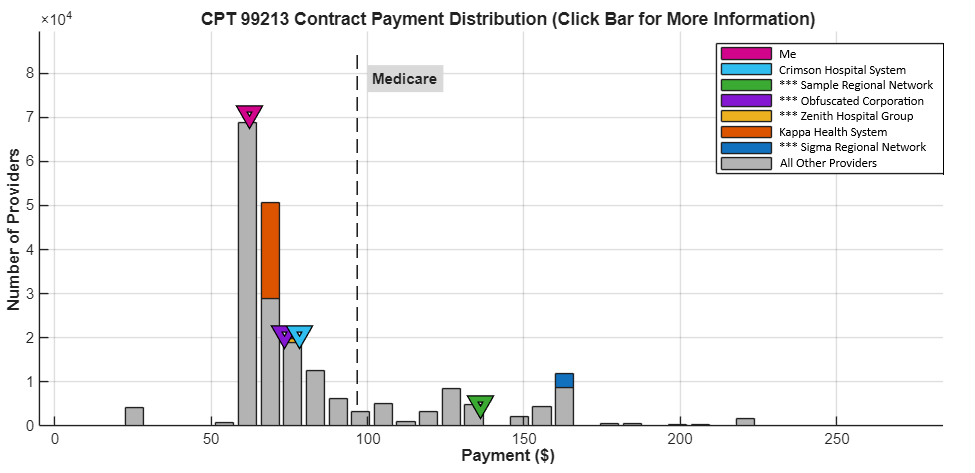
Image: Example “Percent of Medicare” view for a code set
Step 6: Decide on your negotiation mechanism (code level vs conversion factor)
There are two main ways payers can increase reimbursement:
1) Code level adjustments
You pick specific CPTs and request specific new allowed amounts.
Best when:
- a subset of codes is clearly underpaid
- payer refuses broad increases
- your contract structure is messy
2) Across the board increase (conversion factor or fee schedule uplift)
You negotiate an overall percent increase.
Best when:
- you are underpaid across many codes
- you want a simple amendment
- you have leverage and volume
TiC data can support both. But you have to be consistent. If your benchmarks show you are under median on almost everything, asking for a few codes to move may undersell your case.
Step 7: Write the rate increase ask in plain language (template)
Here is a framework you can adapt. Keep it readable. One page is ideal.
Subject: Fee Schedule Adjustment Request, Market Benchmark Support
Summary:
Based on Transparency in Coverage negotiated rate benchmarks for our geography and specialty, our current contracted rates are materially below local market norms across key high volume services.
Findings (high level):
- X of Y benchmarked CPT codes reimburse below the local market median.
- For core E/M codes (list), reimbursement is approximately ___% to ___% below market median.
- This variance creates an estimated annual underpayment of $___ based on our historical volume.
Request:
Effective Sun, 22 Mar 2026 13:43:24 +0000, adjust reimbursement to align with the local market median (or 75th percentile) for the attached CPT set, or apply an equivalent conversion factor increase that results in comparable alignment.
Rationale:
Aligning reimbursement supports continued access for your members, preserves appointment availability, and reflects prevailing contracted rates in our market.
Attachments:
- Benchmark summary report (TiC based)
- CPT list with current rates vs market range
- Utilization and impact summary
Done. Do not write a manifesto.
Step 8: Prepare for the payer’s predictable pushback
They almost always respond with one of these.
“TiC data is unreliable”
Answer: “We use the same data you do – that which your company is required to publish monthly. We agree that the raw data files are complex. That is why we used normalized benchmarks, limited to comparable provider type and geography, and focused on consistent rate signals across multiple contracts.”
Then show them the range and the median. Calmly.
“Those are unique contracts”
Answer: “If these rates are truly non representative, we would like to see your market support for where you believe the median is for comparable providers. Our data indicates otherwise.”
They rarely provide anything.
“We can only offer X%”
Answer: “We can work within constraints. Let’s prioritize the highest impact codes where the variance is greatest, and align those first.”
This keeps you moving.
“We need more time”
Answer: “Understood. Can we set a follow up date now, and can you confirm whether you are reviewing code level alignment or conversion factor options?”
Always leave with a next step. Always.
Step 9: Turn the benchmark into leverage, not just a report
A benchmark report is helpful. Leverage is what changes the outcome.
Leverage can be:
- Access (you are booked out, you are needed)
- Network adequacy (their members need you)
- Performance (quality scores, outcomes)
- Growth (new locations, more covered lives)
- Competitive risk (you may not renew)
TiC data is the anchor. Your leverage is the pressure.
When those combine, that is when rate increases happen.
Common mistakes that quietly kill negotiations
In the realm of negotiations, there are a few recurring pitfalls that can derail the process. Here are some of the most common mistakes to avoid:
- Using benchmarks from the wrong geography. Even one county off can become a distraction.
- Not separating facility vs professional. This can make your numbers look inflated or deflated.
- Benchmarking codes you barely bill. It makes payers think you are fishing.
- Asking for the moon without a path. If you are at 90% of Medicare and you ask for 250% with no story, they will stop taking you seriously.
- No follow up process. Negotiations fail from silence, not rejection.
For a deeper understanding of negotiation strategies and what not to do, consider exploring these negotiation strategies.
Where Reveon Health fits (and why it exists)
Most independent practices do not have access to enterprise level rate intelligence. The data exists publicly, but it is not accessible in practice. It is like someone dumped a warehouse of receipts on the floor and said, “Good luck.”
Reveon Health was launched to close that gap. The platform turns TiC data into specialty focused reimbursement benchmarks designed for payer contract negotiations. Not theory. Not vague market talk. Numbers you can actually use.
If you want to see what TiC based benchmark reporting looks like for your specialty and geography, you can check out Reveon Health here. Even if you do not sign up today, at least get familiar with what “market evidence” can look like when it is clean. It will change how you negotiate.
For more insights on rate negotiations, explore our extensive resources on rate negotiations.
A simple TiC based action plan (do this this week)
If you want the quick version:
- Pick 20 CPTs that drive your revenue.
- Pull your current allowed amounts and volumes for the last 12 months.
- Get TiC benchmarks for your geography and specialty.
- Convert to percent of Medicare or direct dollars, but be consistent.
- Build a 1 page summary with 2 charts and a clear ask.
- Send it, schedule the call, and control the follow up.
That is it. Not easy, but simple.
And the best part is this. Once you do it once, the next negotiation is not scary. It is just process.
Image: Simple one page negotiation summary layout
Closing thought
While TiC data will not magically force a payer to pay you more, it does something almost as important.
It removes the fog.
Instead of “we think we are underpaid,” you walk in with, “Here is the market distribution, here is where you placed us, and here is the correction required.”
That is how you demand a rate increase without sounding demanding at all. You just sound prepared. Which, in payer contracting, is basically a superpower.
FAQs (Frequently Asked Questions)
What is Transparency in Coverage (TiC) data and why is it important for healthcare practices?
Transparency in Coverage (TiC) data consists of public machine-readable files that health plans and issuers are required to post, containing negotiated rate information tied to billing codes. TiC data enables independent healthcare practices to access market-anchored evidence about contracted rates, helping them move beyond relying solely on their own claims experience during payer negotiations.
How can TiC data change the dynamic of fee negotiations with payers?
TiC data shifts negotiation from a subjective plea for higher rates to an objective correction of a variance. By presenting market benchmarks showing that current contracted rates are materially below local norms, practices can demand explanations rather than mere preferences, making the conversation more fact-based and harder for payers to dismiss.
Which CPT codes should practices focus on when using TiC data for benchmarking?
Practices should select a focused list of CPT codes rather than attempting to renegotiate their entire fee schedule at once. Ideal codes include high-volume codes where small rate differences add up, high-revenue codes where even a 10% change is significant, and strategic codes tied closely to the practice’s core services. For example, primary care might focus on office visit codes like 99213–99215 and preventive care codes like 99395–99397.
How should a practice define its ‘market’ when benchmarking rates using TiC data?
Defining ‘market’ carefully is crucial since payers may contest comparability. The market should be defined by geography (such as county or CBSA), provider type (specialty, facility vs professional), billing context (same CPT and relevant modifiers), and plan/product type (commercial PPO, HMO, exchange plans). The closer the match on these factors, the stronger the benchmark’s validity during negotiations.
What challenges exist in accessing and using TiC data directly?
TiC files are often massive (multiple gigabytes), published in varying schemas, missing helpful identifiers, and contain complex rate types requiring interpretation. These factors make manual analysis difficult for most independent practices without dedicated data engineering resources. Specialized tools like Reveon Health have been developed to make TiC-based benchmarks accessible and usable without enterprise-level costs or expertise.
Why is normalizing rates important when comparing your practice’s fees to TiC benchmarks?
Even with clean benchmark numbers from TiC data, direct comparisons can be misleading if not normalized properly. Normalization ensures an apples-to-apples comparison by accounting for differences in coding practices, modifiers, site of service, and plan types. This prevents misinterpretation of data during negotiations and helps maintain credibility with payers.