Stop Using Medicare Multiples: A Better Benchmark
If you have ever been in a payer negotiation where someone says, “We’re at 160 percent of Medicare, so we’re fine,” you already know the problem.
That sentence sounds like a benchmark. It feels clean. Comparable. Almost scientific.
But it’s usually not.
Medicare multiples are one of those habits the healthcare industry picked up because it was convenient. Not because it was accurate. And when you’re making real decisions off it, like whether to accept a renewal, push for a rate increase, or walk away from a payer, “convenient” turns into “expensive.”
This is a piece about why Medicare multiples mislead, what a better benchmark looks like, and how to get there without having to convert your team into a mini analytics firm.
The appeal of Medicare multiples (and why everyone keeps using them)
Medicare is public, consistent, and easy to reference. That’s basically it. It’s a known fee schedule, updated annually, and it gives you a tidy index to hang your commercial rates on.
So you end up with stuff like:
- Payer A pays 145 percent of Medicare for office visits
- Payer B pays 175 percent of Medicare for the same set
- Therefore Payer B is better
And sometimes, sure, it points you in the right direction.
But the real reason it caught on is because it saves time. It lets people benchmark without dealing with actual market rates. No one has to parse messy contracts. No one has to figure out what “the market” is. No one has to memorize dozens of payment rates for different CPT codes. You just compare your Medicare multiple, shrug, and move on.
The issue is that negotiations are not happening against Medicare. They are happening against other commercial payers in your market, paying real allowed amounts, under real contracts, with real quirks.
Which Medicare does not reflect.
Why Medicare multiples break down in real negotiations
Let’s walk through the big reasons, the ones that actually show up in negotiation calls and renewal reviews.
1. Medicare isn’t the market. It’s a policy tool.
Medicare rates are shaped by federal policy goals, geographic adjustments, and budget neutrality rules. They’re not designed to represent what commercial payers will pay. They’re not even designed to represent cost.
So when a payer tells you, “We pay 170 percent of Medicare,” that might be generous. Or it might be below market. It depends on specialty, CPT mix, geography, setting, and what commercial contracts around you look like.
Medicare gives you a single anchor. The market is not anchored that way.
2. The multiple hides CPT level distortion
Here’s a quiet truth. The “multiple” is almost always calculated on a blended set of codes. Sometimes it’s a basket of common CPTs. Sometimes it’s historical utilization. Sometimes it’s just whatever someone grabbed quickly.
Blending creates a problem: payers can be strong on a few low volume codes and weak on the ones that actually matter to your margin.
So you end up “at 160 percent” while:
- your key procedural codes are underpaid
- your injectables administration is oddly low
- your new patient visits are fine, but your follow ups are terrible
- your imaging reads are lagging, and no one noticed because the blended multiple looked okay
Take a look at the example below. 172% Medicare Multiple sounds great on paper, but if your billing mix heavily weights E/M codes, you might only observe 130% Medicare.
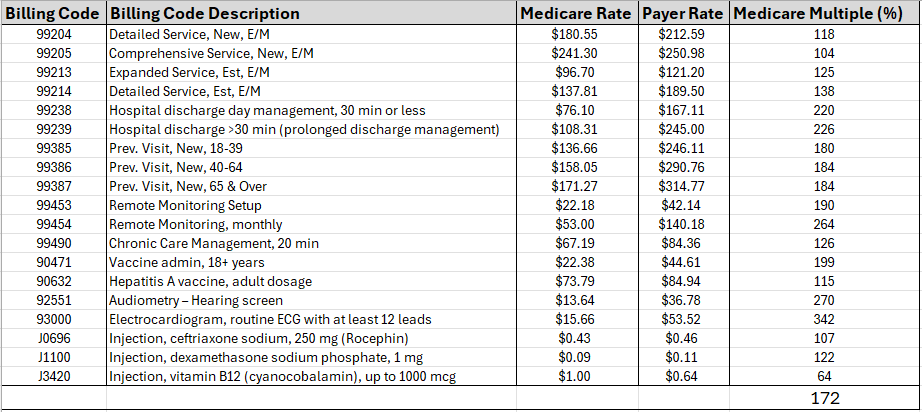
The multiple smooths out the pain (and the details). In negotiation, smoothing is the enemy.
3. Medicare differentials don’t match commercial differentials
Commercial payers don’t always value codes the way Medicare does, especially once you get into specialty heavy areas and site of service nuances.
Also, commercial contracts can include:
- carve outs
- case rates
- different modifier policies
- multiple procedure reduction rules
- bundled payment logic that isn’t consistent with Medicare
So even if you’re “a multiple of Medicare,” that doesn’t tell you what you are actually getting paid relative to the commercial environment.
4. Geography gets weird fast
Medicare has geographic adjustments, sure. But they do not mirror commercial network dynamics in your metro, your county, or even your zip level catchment. Our recently published article, A Transparency-in-Coverage (TiC) Data Analysis of the Negotiated Commercial Rates for CPT 99213, Normalized to Medicare, shows substantial variation in Medicare multiple across states and regions in the country.
Two practices within the same state can have totally different payer dynamics because:
- one is the only specialty group in a 40 mile radius
- one is in a dense market with three health systems competing
- one has access to a high demand sub specialty niche
- one is essentially a commodity provider in that payer’s eyes
Medicare multiples don’t see any of that.
5. Payers know you’re using it, and they use it back
This is the frustrating part. Medicare multiples are not neutral. Payers understand how many provider groups use them as a shortcut. So the payer will frame the deal that way.
They’ll say things like:
- “You’re already above 150 percent of Medicare, which is strong for your area.”
- “We can’t justify 200 percent of Medicare.”
- “This is aligned with Medicare based contracts across our network.”
Even when the actual commercial market rates in your region suggest something very different.
If you don’t have a market grounded counterpoint, the conversation stays in their frame.
So what should you benchmark against instead?
A better benchmark is simple to say, harder to do:
Benchmark against commercial allowed amounts in your local market for your specialty and CPT mix.
Not a national average. Not Medicare. Not a vague “usual and customary.” Not what someone heard at a conference.
Actual negotiated rates, in your region, for the codes you care about.
That’s the only thing that answers the questions you’re really asking:
- Are we underpaid relative to other providers around us?
- Which CPT codes are dragging our contract down?
- Where are the biggest opportunities by payer?
- If we push for an increase, what is a defensible ask?
- What does the payer already pay others in our geography?
This is where Transparency in Coverage data becomes a game changer, because it contains payer published negotiated rate information. It’s messy data, yes. But it is the closest thing we’ve ever had to a broad commercial market reference.
And that’s what Reveon Health is built around.
The benchmark that works in the real world: “Market rate opportunity by CPT”
When we say “better benchmark,” it’s not just “compare yourself to the market.” It’s how you compare.
The most useful benchmark looks more like this:
- Pick your priority CPT codes (the ones you bill often, and the ones that drive revenue)
- Look at commercial negotiated rates for those codes in your geography
- Segment by payer and sometimes product lines when available
- Compare your contracted allowed amounts to the market distribution
- Quantify the opportunity: dollars per service, expected annual impact, and negotiation targets
That’s negotiation ready. That’s something you can put into a deck, a renewal memo, or a call script.
It also prevents the classic trap where you ask for “a 12 percent increase across the board” because you don’t know where the real gap is.
Sometimes the best move is to ask for targeted increases on 8 codes, not a blanket bump.
A quick example (a realistic one)
Say you’re a specialty practice and your top 15 CPTs represent 70 percent of your professional revenue.
You look at Payer X and you find:
- You’re competitive on evaluation and management codes
- But you’re 18 to 25 percent below market on three procedure codes that you do all day
- The payer’s negotiated rates for those same codes in your county cluster higher for other providers
If you only used a Medicare multiple, you might think you’re fine. Especially if the E/M codes are strong.
But with market benchmarking, the story becomes:
- “We’re at or above market on E/M, agreed.”
- “But on these specific procedure codes, we are materially under market in this region.”
- “Here is the market range, here is where we sit, here is the rate we are requesting, and here is the annualized impact based on volume.”
Now it’s not an emotional negotiation. It’s a documentation exercise.
That shift matters.
What makes a benchmark actually credible to a payer?
This part is subtle, but it’s where negotiations often succeed or stall.
A payer will ignore a benchmark if it’s:
- vague
- not local
- not code specific
- not defensible
- not tied to contracted allowed amounts
A payer is more likely to engage when you bring:
- geography aligned comps (state is often too broad, metro or county is better)
- your specialty matched to the benchmark set
- code level negotiated rate distributions
- clear citations and methodology, at least enough to show it’s not made up
- a specific ask that maps to the data
This is exactly why “Medicare multiple” arguments tend to go nowhere. They’re too easy to dismiss.
The practical problem: Most teams don’t have time to do this
Even if you agree with everything above, you might be thinking, okay, but who is actually going to pull TiC data, normalize it, filter it by payer and geography, and turn it into something negotiation usable?
Most practices are already stretched. Even many RCM teams and consulting groups end up doing half measures because the data workflow is brutal.
This is where Reveon Health is intentionally different.
Reveon Health provides specialty specific commercial payer reimbursement benchmark reports built from Transparency in Coverage data, and the point is that you do not have to build the analytics machine yourself.
You submit a few key inputs, stuff you already know:
- NPI
- specialty
- payer(s)
- geography
- priority CPT codes
Then you get a free rate opportunity screen. If it looks useful, you can order the full report.
The big value is not just the data. It’s that the report is:
- done for you
- negotiation oriented
- quality checked by specialists
- designed to be affordable enough that smaller practices are not locked out of market intelligence
That last part matters more than people admit. Too much of this industry assumes only big systems get access to rate truth.
What you should stop saying in negotiations (and what to say instead)
Here are a few swaps that immediately make your negotiation posture stronger.
Stop saying: “We need 200 percent of Medicare.”
Say: “We are under market for these priority CPT codes in this geography, and we are requesting alignment to the local negotiated rate range.”
Because the first statement is easy to dismiss. The second forces a real response.
Stop saying: “We’re below where we should be.”
Say: “For CPT 12345 and 67890, our allowed amounts are X. The market distribution in this area for this payer is Y to Z. We are requesting Y.”
Specificity changes the whole tone of the call.
Stop saying: “We want a across the board increase.”
Say: “We are requesting targeted adjustments on the codes that are most misaligned and highest volume. We can keep other sections stable.”
This makes it easier for the payer to say yes, and it keeps you from accidentally giving away something else in the contract.
But wait, are Medicare multiples ever useful?
Yes. A little.
Medicare multiples can still be a quick internal sanity check. They can help when:
- you’re doing a first pass review and have nothing else
- you’re comparing two contracts within your own organization, same CPT mix
- you’re looking at a single code where Medicare valuation roughly tracks commercial patterns
But they should not be your primary benchmark for market positioning.
Think of Medicare multiples like BMI. Fine as a rough flag. Terrible as a full health assessment.
How to move off Medicare multiples without causing chaos
You do not need to overhaul everything overnight. You just need to change what you treat as “truth.”
A simple path:
- Pick 10 to 25 CPT codes that matter most (volume plus margin).
- Benchmark those codes commercially by payer and geography.
- Use that to set negotiation targets, not a blanket multiple.
- Repeat quarterly or before renewals, not once every three years.
If your team can’t realistically do step 2 in house, that’s the moment to bring in a done-for-you benchmark report.
That’s literally what Reveon Health is for.
If you want to see what this looks like for your own practice, start with the free screen and keep it simple. Your top CPTs, your top payers, your real geography. Then decide if a full report is worth it.
You can request your free screen here: https://reveonhealth.com/request-a-report
The real takeaway
Medicare multiples are comforting because they’re easy. That’s the problem.
Commercial payer negotiations are local, code specific, and market driven. Your benchmark should be the same.
If you want stronger negotiations, fewer blind spots, and a faster path to “here is our ask and here is why,” stop benchmarking against Medicare and start benchmarking against the commercial market you actually live in.
And if you want it without building a whole analytics workflow, that’s the niche Reveon Health is carving out. Affordable, specialty specific, negotiation ready benchmark reports. Built from TiC data. Checked by people who do this all day.
That’s the better benchmark.
FAQs (Frequently Asked Questions)
Why are Medicare multiples commonly used as benchmarks in payer negotiations?
Medicare multiples are popular because Medicare rates are public, consistent, and easy to reference. They provide a known fee schedule updated annually, allowing providers to benchmark commercial rates conveniently without parsing complex contracts or defining the market.
What are the main problems with using Medicare multiples as a benchmark in commercial payer negotiations?
Medicare multiples often mislead because Medicare rates are policy-driven and not reflective of commercial market rates. They hide distortions at the CPT code level, don’t match commercial differentials, fail to capture local geographic payer dynamics, and payers themselves use these multiples strategically during negotiations.
How does blending CPT codes affect the accuracy of Medicare multiple benchmarks?
Blending CPT codes creates a distorted picture because it averages payments across various codes. Payers might pay well on some high-volume codes but underpay crucial procedural or follow-up codes. This smoothing effect can mask true underpayments that impact margins negatively.
Why don’t Medicare rate differentials align with commercial payer valuations?
Commercial payers value codes differently than Medicare, especially in specialty areas and site-of-service contexts. Commercial contracts may include carve outs, case rates, modifier policies, procedure reductions, and bundled payment models that differ significantly from Medicare’s approach.
How do geographic factors influence the reliability of Medicare multiples as benchmarks?
Medicare adjusts rates geographically based on federal rules but these adjustments don’t reflect actual commercial network dynamics within metros, counties, or zip codes. Market competition, specialty availability, and provider uniqueness cause significant variation that Medicare multiples overlook.
What is a better approach to benchmarking payer contracts instead of relying on Medicare multiples?
A superior benchmark involves analyzing commercial allowed amounts in your local market specific to your specialty and service mix. This requires understanding real contract terms and market dynamics rather than defaulting to convenient but inaccurate Medicare-based multiples.