Denials + Reimbursement Intelligence: The Missing Link in RCM Strategy
“We need to reduce denials.
We need faster A/R.
We need better collections.”
All true. Also kind of incomplete.
Because denials management, by itself, is often treated like a cleanup crew. You chase down rejections, appeal what you can, write off what you cannot, and hope next month is calmer. Meanwhile, the real engine behind a lot of denials and underpayments sits quietly in the background.
Your contracted rates.
Your fee schedule logic.
Your payer behavior at the CPT and modifier level.
And if you do not have clean reimbursement intelligence, you are fighting in the dark. You might win some appeals. You might reduce a few avoidable denials. But you will keep missing the bigger story.
Reimbursement intelligence is the missing link to recover costs from denials. It turns denials from a reactive workflow into a strategic signal.
This is where Transparency in Coverage data and analytics, when used correctly, stops being a buzzword and starts becoming a practical tool for RCM teams, managed care negotiators, PMS platforms, and the RCM firms supporting thousands of independent practices.
Why denials alone will never fix your revenue problem
Denials management is necessary. But it is not sufficient.
A denial is just an outcome. The cause could be any of these:
- Eligibility was wrong or not captured at time of service.
- Authorization rules changed, or were applied inconsistently.
- Coding is correct, but payer policy edits are stricter than expected.
- The payer processed the claim, but paid at a lower rate than your team assumed.
- The payer processed correctly, and the rate is… unfortunately, exactly what you signed.
That last one is the quiet killer. It is not a denial. It is a contract issue wearing an RCM costume.
RCM teams often lump “underpayment” into the denials bucket, because operationally it feels similar. Someone has to work it. Someone has to call. Someone has to appeal. But if the payer is paying according to contract, appeals do not fix it. Negotiation fixes it.
And the fastest way to tell the difference is having reimbursement intelligence that is specific, local, specialty aware, and payer specific.
Not vibes. Not what the practice “usually gets.” Real benchmarks and contract rate context.
The blind spot: RCM teams are optimizing claims without knowing the price
Let’s say you reduce your denial rate from 12% to 8%. That is a win.
But what if, during the same period, you are being paid 18% below market on a cluster of high volume codes because the contract is outdated?
Then you are basically running a more efficient engine… that is still selling your services at a discount.
This happens all the time, especially with independent practices that do not have:
- in house contract analysts,
- clean fee schedule repositories,
- a way to compare negotiated rates to peers,
- or enough leverage to push payers without proof.
So you see RCM firms doing heroic work, squeezing down preventable denials, only to discover later the “real revenue” was locked behind payer contracting. Which the RCM team was not resourced to tackle.
That is where reimbursement intelligence changes the whole game.
What “reimbursement intelligence” actually means in an RCM context
This is not just “we have a contract.”
Reimbursement intelligence is the ability to answer, quickly and credibly:
- What should this code pay, under this payer, in this geography, for this specialty?
- Is the payment variance explained by contract, policy, bundling, modifier rules, place of service, or something else?
- Are we losing money because of preventable denials, or because our baseline negotiated rates are weak?
- Which payers are consistent underpayers vs. simply strict on edits?
- Which codes represent the biggest negotiation opportunity?
You can build some of this with internal data. But internal data has a problem. It only tells you what you have been paid, not what you could be paid.
Benchmarks matter. External reference points matter. Especially in contract negotiation and payer escalation.
Transparency in Coverage (TiC) data is the underused piece here
TiC data is messy. Huge files, weird formats, hard to interpret. So most organizations either ignore it or treat it like a compliance artifact.
But TiC data contains payer published negotiated rates. When you turn that raw data into usable analytics, you get something RCM teams almost never have at scale.
A view into reimbursement norms and pricing gaps across payers, codes, specialties, and regions.
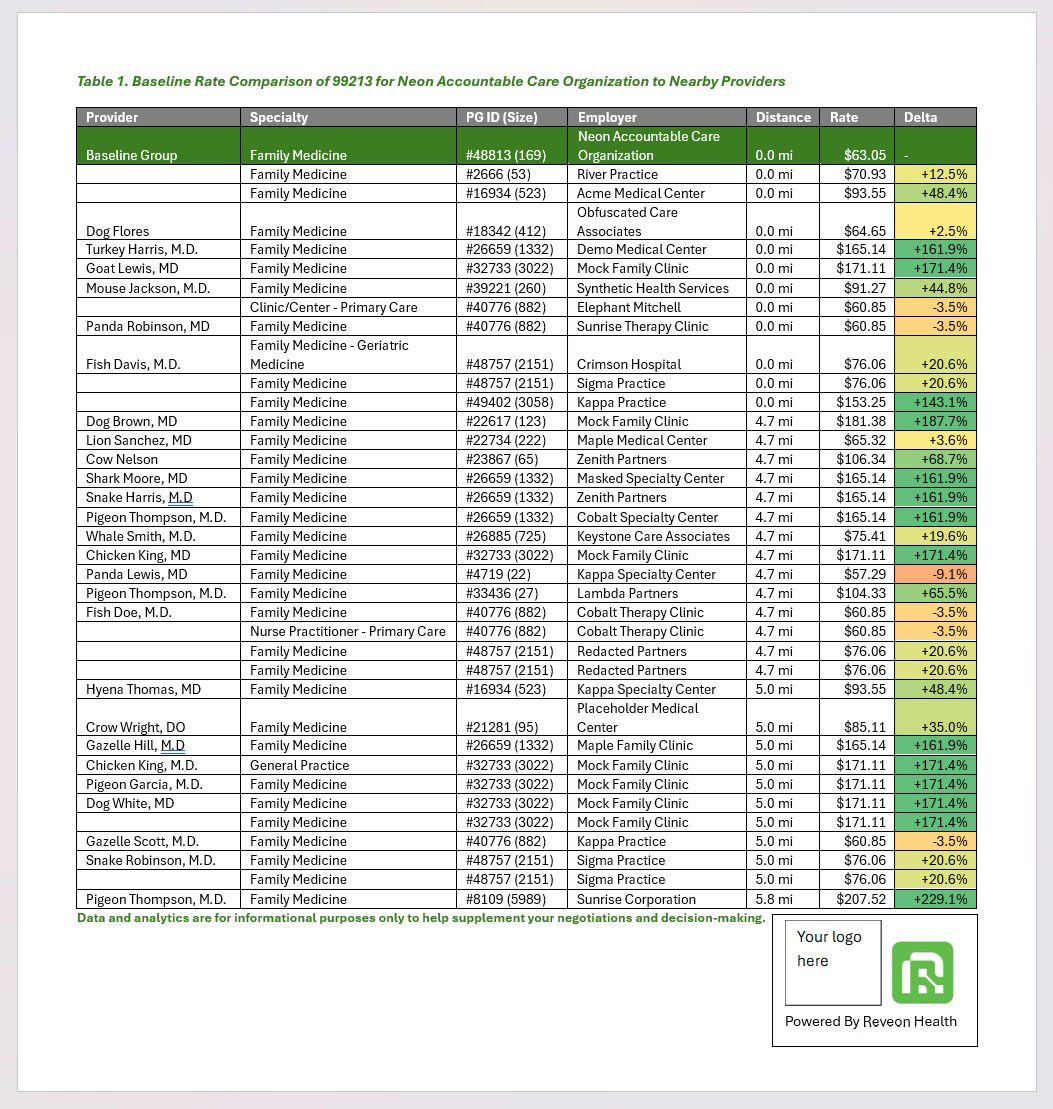
That is the core idea behind Reveon Health: a web based analytics platform that turns TiC machine readable files into clear, specialty focused benchmark insights, so providers and the organizations supporting them can spot underpayment risk and negotiate smarter.
And in the denials world, those insights are not “nice to have.” They let you triage the work correctly.
Denials data tells you what happened. Reimbursement intelligence tells you why it keeps happening.
Here is a simple way to think about it.
Denials analytics answers:
- What was denied?
- What are the top denial reasons?
- Which locations, providers, or billers are driving them?
- How long to resolve?
- What is the overturn rate?
Reimbursement intelligence answers:
- Was the claim ever profitable at the contracted rate?
- Is the denial pattern tied to payer policy that is effectively a reimbursement reduction?
- Is this payer paying below benchmark even when clean?
- Are we seeing systematic downcoding, bundling, or modifier suppression?
Put them together and you get something powerful.
A denial is no longer just an operational fire. It becomes a payer signal. A contract signal. A negotiation signal.
The “appeal treadmill” and how to get off it
Many RCM teams live on the appeal treadmill.
They win enough appeals to justify the labor. Then the payer keeps denying the same way next week. The team adds more staff. Or burns out. Or both.
Here is the uncomfortable truth: some denial categories are basically soft denials.
Not formally denied. But reduced, delayed, or manipulated through adjudication rules that are hard to contest. Examples:
- “Bundled per NCCI” when peers are paid separately under other contracts.
- Modifier 25 or 59 suppression patterns.
- Multiple procedure reductions that exceed what you see elsewhere.
- “Not medically necessary” tied to opaque payer policies.
- Downcoding patterns on E/M.
Sometimes you can fix documentation and coding. Sure.
But sometimes you are seeing a payer behavior pattern that is only fixable with contract language changes, policy carve outs, fee schedule updates, or escalations supported by benchmark proof.
That last part is where TiC based benchmarking can strengthen the case. If you can credibly show, code by code, that the payer is out of line relative to other negotiated rates in the market, you move the conversation from opinion to evidence.
A practical model: the Denials + Rate Intelligence loop
If you are building a modern RCM strategy, the loop looks like this:
- Identify top denial and underpayment categories by dollars, not volume.
- Classify whether the root cause is operational (front end), clinical/coding, or contractual.
- Benchmark reimbursement for the impacted CPT set, by payer and geography.
- Decide the play: workflow fix, coding education, targeted appeal, payer escalation, or contract negotiation.
- Measure post fix results, and repeat.
This is not theoretical. It is how you stop treating denials as random noise.
Where this matters most: independent practices and the firms that support them
Large health systems can sometimes brute force this with teams and tools.
Independent practices cannot. They rely heavily on outside partners:
- RCM firms
- managed care contracting groups
- practice management and billing platforms
- clearinghouses and revenue cycle tech vendors
Those partners already have distribution. They have trust. They have workflows.
What they often lack is a scalable, credible reimbursement benchmarking layer that fits inside what they already do.
So a practice asks, “Are we being underpaid?” and the partner can only answer with internal experience. Or a gut check. Or an expensive consulting project.
This is exactly the gap TiC driven analytics can fill, especially as a white label or embedded product.
The partnership angle: why RCM companies should care
If you are an RCM organization, adding reimbursement intelligence does a few things for you immediately.
1. It changes your value proposition
Instead of “we reduce denials and collect faster,” it becomes:
We reduce denials, and we identify contract and reimbursement gaps that your practice did not even know existed.
That is a stronger story. And it is easier to defend during renewals.
2. It makes your denials work smarter
Not all denials deserve the same effort.
If a CPT is reimbursed poorly relative to benchmark, you may prioritize negotiation over endless appeals. Or you may decide the real fix is steering volume, changing scheduling, or revisiting payer participation.
Rate context helps you allocate labor.
3. It creates a new revenue line
Benchmark reports, underpayment audits, payer scorecards, contract optimization packages. These are natural expansions that many RCM firms want, but struggle to scale because the data is hard.
4. It deepens stickiness with clients
Once a practice sees its payer rate gaps in black and white, it is hard to unsee. It becomes part of quarterly business reviews. Part of strategy, not just billing.
The same is true for managed care negotiators
Negotiators already know this, but they often lack fast benchmarking at the code level. They might have:
- charge master comparisons,
- broad “rate increase” targets,
- payer messaging,
- maybe a third party benchmark source that is expensive or slow.
TiC derived negotiated rate insights can support:
- prioritization: which payer and which codes matter most,
- evidence: what peers are seeing,
- targeting: where fee schedule uplift will hit the bottom line,
- and timing: when to push, renew, or escalate.
And if you are serving many independent practices, having a repeatable data product matters. It keeps negotiation from being bespoke every time.
What to look for in a reimbursement intelligence partner (and what to avoid)
If you are considering a TiC analytics partner or white label solution, a few things matter more than flashy dashboards.
- Specialty focused views. Primary care needs different code sets than ortho, GI, or behavioral health.
- Geographic relevance. A national average is not useful if you negotiate locally.
- CPT level clarity. High volume and high impact codes should be obvious.
- Payer specificity. “Commercial” is not a payer. You need plan level detail.
- Usability for non analysts. If it takes a data team to interpret, it will not scale.
- Integration options. RCM and PMS firms need API or export ready workflows.
- Defensible sourcing. TiC data is public, but the processing and normalization is the real work.
Also avoid the trap of thinking benchmarking replaces contract knowledge. It does not. It complements it. The goal is to give your RCM and contracting teams leverage and focus.
Incorporating strategies such as those suggested by Reveon Health, can further enhance your revenue generation efforts through effective medical billing strategies and optimizing reimbursement processes.
A simple scenario where this changes the outcome
Imagine a 4 provider cardiology practice.
They complain about denials from Payer X. The RCM team digs in and finds:
- a high rate of modifier related denials,
- plus a pattern of reduced payment even when claims are clean.
Without reimbursement intelligence, the team may assume the reduced payments are correct. Or spend months appealing without knowing if it is worth it.
With a benchmark view, you might find:
- Payer X is paying significantly below market on a handful of core CPTs.
- Even if you win every denial, the baseline reimbursement is still weak.
- Competitor payers in the same market reimburse higher for those services.
Now the play changes.
Yes, fix the modifier workflow. But also, open a contract conversation with a specific fee schedule uplift target tied to a defined CPT list. And when you escalate, you bring data.
So where does Reveon Health fit into this?
Reveon Health is building exactly the reimbursement intelligence layer that many RCM, managed care, and PMS organizations want to offer their clients, without having to build TiC ingestion and normalization themselves.
It is a web based analytics platform that converts payer TiC files into specialty focused reimbursement benchmark reports, helping identify:
- negotiated rate gaps,
- underpayment risk,
- and smarter negotiation targets.
This platform not only aids in understanding how provider groups dictate your reimbursement, but also provides insights that can be crucial when dealing with hospital system referrals and their impact on reimbursement.
And because the platform is built for self serve access and scalable reporting, it is a natural fit for B2B partnerships that want to add:
- white label benchmark reports,
- embedded reimbursement insights,
- or integrated workflows for contract and payer performance analysis.
If you are an RCM firm, managed care negotiation group, or a PMS vendor supporting independent practices, you can explore what this looks like by signing up for a free demo video, requesting sample reports, or contacting us with any questions you might have.
The takeaway (the part to actually act on)
If your RCM strategy is only focused on denials, you are leaving money on the table in a way that is hard to see from inside the claims workflow.
Denials are symptoms.
Reimbursement intelligence is context.
Put them together and you get a system that can:
- reduce avoidable denials,
- stop wasting labor on unwinnable fights,
- identify payer behaviors that require escalation,
- and surface contract gaps that quietly drain revenue every month.
And for organizations like RCM firms, contracting groups, and PMS platforms that sit upstream of thousands of small practices, this is also a product opportunity. A way to expand what you offer, with data that clients immediately understand.
Denials plus reimbursement intelligence is not an extra dashboard.
It is the missing link.
FAQs (Frequently Asked Questions)
Why is managing denials alone insufficient to fix revenue problems in healthcare RCM?
Managing denials is necessary but not sufficient because a denial is just an outcome. The underlying causes can include eligibility errors, authorization changes, stricter payer policies, or contract issues leading to underpayment. Without addressing these root causes—especially contract-related reimbursement issues—denials management alone cannot fully resolve revenue challenges.
What role does reimbursement intelligence play in improving revenue cycle management (RCM)?
Reimbursement intelligence provides specific, local, specialty-aware, and payer-specific insights into contracted rates and fee schedules. It helps RCM teams understand whether payment variances are due to contracts, policies, or coding issues. This intelligence transforms denials from reactive cleanup into strategic signals for negotiation and optimization, enabling better revenue outcomes.
How can Transparency in Coverage (TiC) data enhance RCM strategies?
Transparency in Coverage (TiC) data contains payer-published negotiated rates that, when properly analyzed, offer valuable benchmarks across payers, codes, specialties, and regions. Utilizing TiC data through platforms like Reveon Health allows providers to identify underpayment risks and negotiate smarter contracts, turning TiC from a compliance artifact into a practical tool for RCM improvement.
What are common blind spots RCM teams face when optimizing claims without reimbursement intelligence?
Without reimbursement intelligence, RCM teams may reduce denial rates but still get paid significantly below market rates due to outdated contracts or lack of benchmarking. They often lack in-house contract analysts, clean fee schedule repositories, and leverage to push payers effectively. This leads to optimized claims processing but missed opportunities for higher revenue through better contracting.
How do denials analytics differ from reimbursement intelligence in the context of RCM?
Denials analytics focus on what happened: identifying denied claims, top denial reasons, responsible locations or providers, resolution times, and overturn rates. Reimbursement intelligence explains why denials or underpayments occur by assessing claim profitability at contracted rates, payer payment patterns versus benchmarks, and systematic coding or bundling issues. Together they provide a comprehensive view of revenue challenges.
What key questions should reimbursement intelligence answer for effective RCM?
Effective reimbursement intelligence should quickly answer: What should this code pay under this payer in this geography and specialty? Is payment variance due to contract terms, policy edits, bundling rules, or place of service? Are losses due to preventable denials or weak baseline negotiated rates? Which payers consistently underpay? And which codes offer the biggest negotiation opportunities?